|
__________
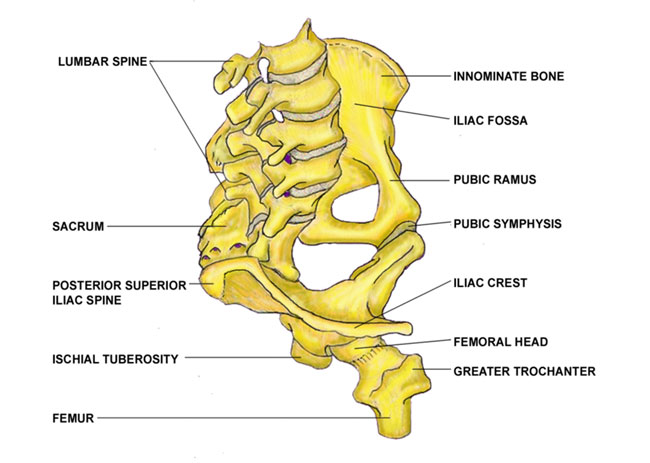
Basic Anatomy
Bones
The pelvic ring is composed of two innominate bones and the sacrum.

click to
enlarge
Personal injury attorneys in Anaheim
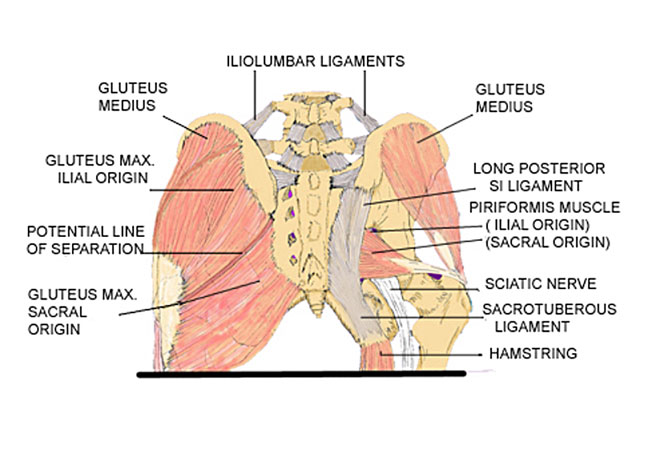
Principal Muscles
and Ligaments

click
to enlarge
Innervation
The innervation to the sacroiliac joints is highly variable and
complex. Pain may be referred in a sclerotomal fashion. Adjacent
structures may be affected by intrinsic joint pathology and become
active nociceptors. Pain referral patterns may be dependent on the
distinct locations of injury to the sacroiliac joint. The anterior
portion of the sacroiliac joint receives innervation from the posterior
rami of the L2-S2 roots, but these contributions are highly variable
and may differ in the joints of a given individual.
Additional innervation to the anterior joint may arise directly
from the obturator nerve, the superior gluteal nerve, and the lumbosacral
trunk. The posterior portion of the joint is innervated by the posterior
rami of L4-S3.
An additional autonomic component of the innervation to the sacroiliac
joint further increases the complexity of its neural supply and
likely adds to the variability of the pain referral patterns.
The sciatic nerve passes immediately beneath or traverses through
the piriformis and may become irritated by spasm of the piriformis.
back to top
__________
The Sacroiliac Joints
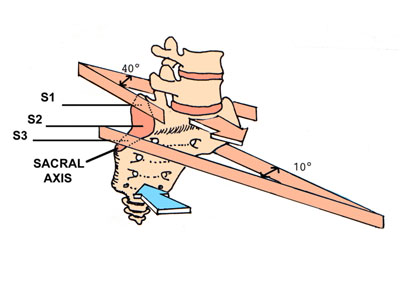
Angles (from Solonen)
The unique shape of the joint is essential to normal function.
Form follows function

click
to enlarge
Joint Angulations and Loading on the Sacral Axis
Loading is anterior and takes place on a sacral axis at the most
posterior part of the S3 sacral
segment of the sacroiliac joint. Note the shape at S1 and how it
is prone to 'fall away' from the ilial joint surface with ligamentous
loading.
click
to enlarge
back to top
__________
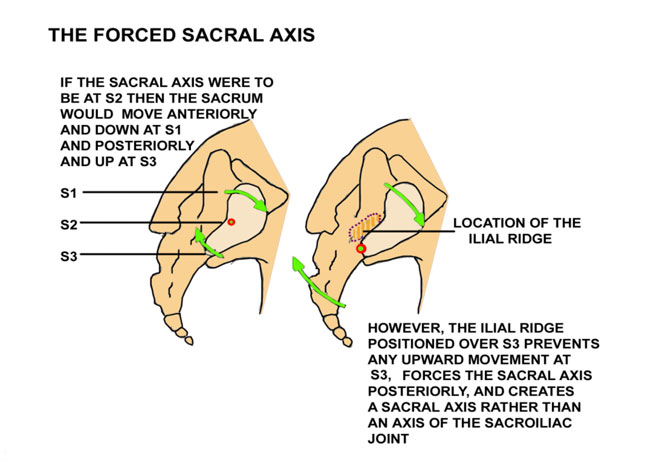
The Forced Sacral Axis
The ilial ridge just cephalad to the
S3 sacral segment prevents any cephalic movement at S3 and forces
the location of the axis to the posterior aspect of S3. A bony
transition
point at that location has been
verified by Gracovetsky.

click
to enlarge
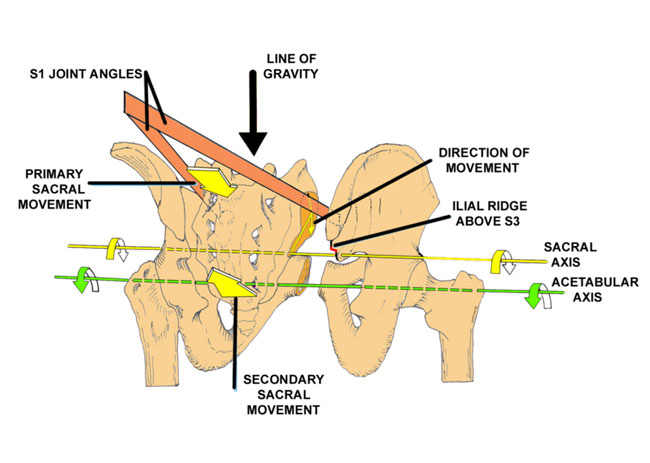
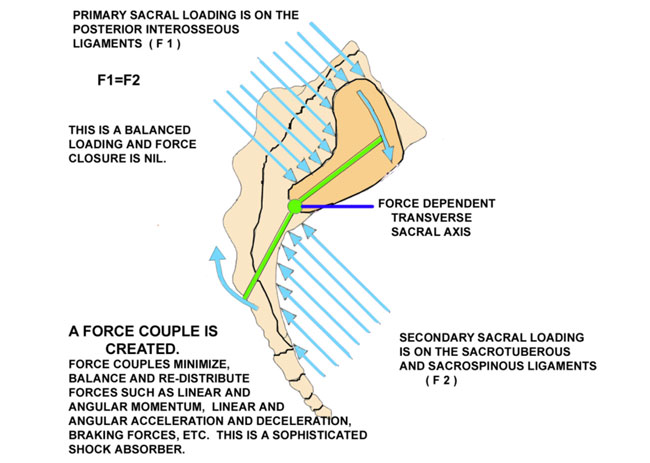
Primary and Secondary Loading on the Sacral Axis
Primary sacral loading is on the posterior interosseous ligaments.
Secondary loading is
on the sacrotuberous and sacrospinous ligaments. The secondary
loading will equal, but cannot
exceed the primary loading. Sacral loading increases the lumbar
lordosis and the lumbosacral
angle.
The ilial ridge forces the sacral axis by not
allowing any cephalic movement of the
sacrum on the innominate bone or any normal or pathological caudad
movement of the
innominate bone on the sacrum. Posterior rotation of the innominate
on the sacrum can
only occur with correction when the joint is already in dysfunction. 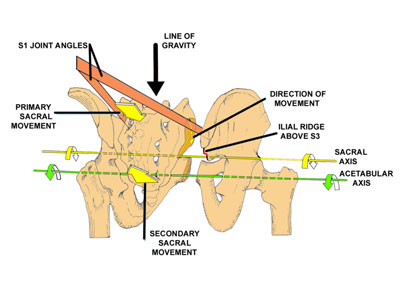
click
to enlarge
back to top
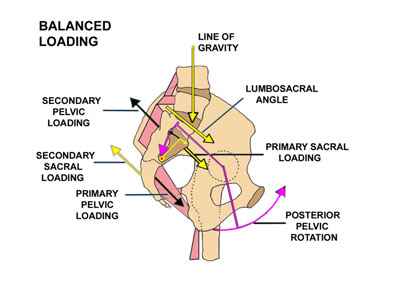
Primary and Secondary Pelvic Loading on the Acetabular Axis
Vleeming described form closure, force closure and self-bracing
in the sacroiliac joint, but this can
only occur in the unloaded pelvis or in the pelvis of the fresh
cadaver. WHEN THE JOINT IS LOADED EVERYTHING CHANGES. NEITHER FORM
NOR FORCE CLOSURE NOR SELF-BRACING CAN
OCCUR WHEN THE JOINT IS LOADED WITH THE SUPERINCUMBENT WEIGHT.
After loading, the line of gravity is
anterior to the sacral axis, but posterior to the acetabula causing
a posterior pelvic rotation
and creating a dynamic, balanced tension on the pelvic ligaments. The posterior pelvic rotation decreases the lumbar lordosis and
the lumbosacral angle.
The sacroiliac joints are vulnerable to injury through minor and
major trauma with an
anterior shift in the line of gravity causing an anterior rotation
of the innominate bones on the sacrum with a reversible subluxation
and fixation.
500','yes');return false;">click
to enlarge
DonTigny ©
The Force Couple
The opposing forces created when the ligaments are loaded create
a force couple. The moment
created by the force couple creates a force-dependent transverse
axis of rotation for the sacroiliac joints.

click
to enlarge
DonTigny ©
back to top
__________
Biomechanics
Sacral Movement on the Asymmetric Pelvis With Normal Ambulation

click
to enlarge
DonTigny ©
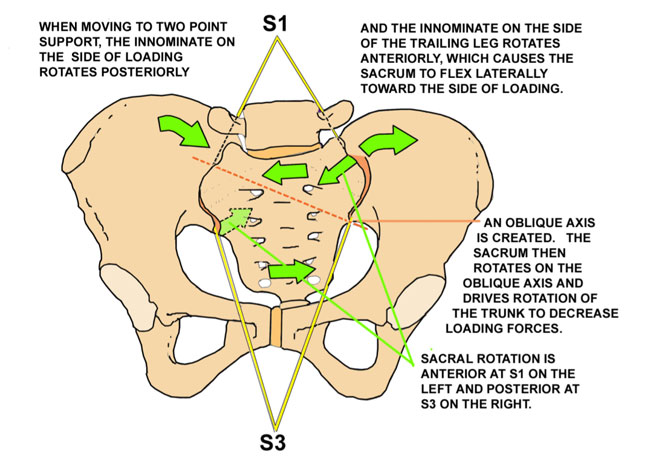
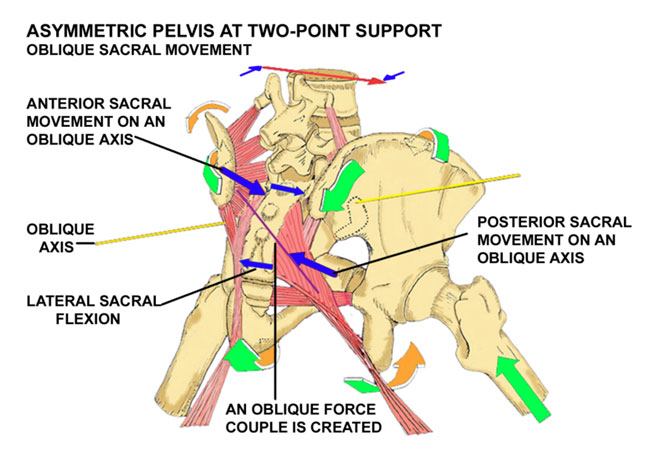
Oblique Sacral Movement on the Oblique Sacral Axis
The weight of the superincumbent trunk anterior to the oblique
sacral axis at S3 on the left causes
a sacral movement anteriorly at S1 on the left and posteriorly
at S3 on the right just as soon as the normal
axis on the symmetric pelvis begins to move into asymmetry. The
sacrotuberous ligament is helical and
allows this movement.
The longer the stride, the greater is the asymmetry, the greater
is the lateral sacral flexion and thus
the greater the sacral rotation on the oblique axis. An oblique
force couple is created from the posterior interosseous ligament
on the left to the sacrotuberous ligament on the right. The sacral
rotation drives trunk rotation toward the right (the side of loading),
precedes the loading and serves to decrease the impact loading.

click
to enlarge
DonTigny ©
back to top
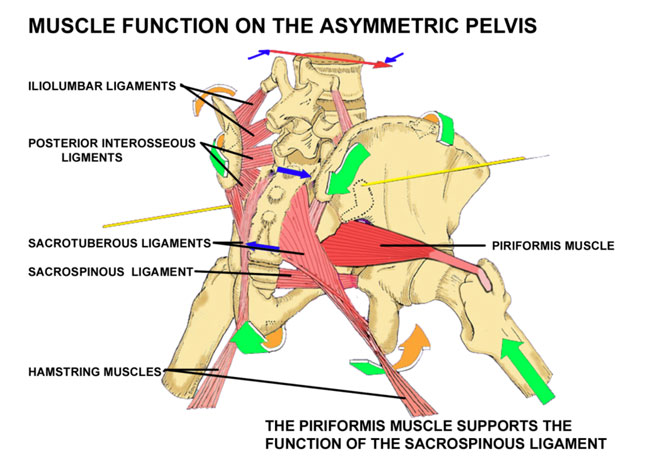
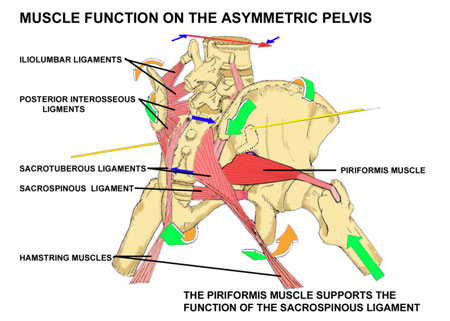
Piriformis Function
The piriformis muscle functions to support and assist the sacrospinous
ligament in restoring
the sacrum to its resting position as the pelvis moves to a position
of symmetry at mid-step.
click
to enlarge
DonTigny ©
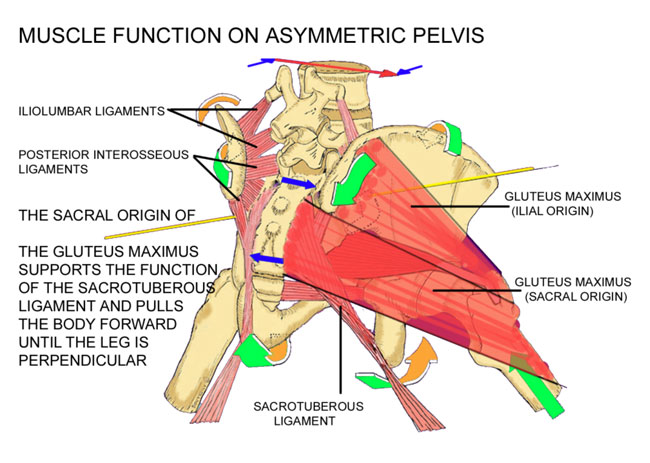
Function of the Gluteus Maximus
The sacral origin of the gluteus maximus serves to assist and support
the function of the
sacrotuberous ligament in bringing the distal sacrum anteriorly
and laterally as the sacrum moves
from lateral flexion to its resting position when the pelvis moves
to symmetry at mid-step. This is
necessary because the superincumbent weight is all anterior to
the sacral axis and the sacrotuberous
ligament is on stretch. The sacral origin of the gluteus maximus
and the piriformis must act
as prime movers on the sacroiliac joint when the pelvis is asymmetrical.
The sacral origin of the gluteus maximus also functions to pull
the pelvis anteriorly over the
loaded side until the leg is perpendicular at mid-step. The
ilial origin of the gluteus maximus then
undergoes an eccentric contraction to decrease the loading forces
on the contralateral side.

click
to enlarge
DonTigny ©
back to top
BIOTENSEGRITY
The biomechanical concepts I have described are consistent with
current biotensegrity concepts.
There are at least ten pelvic rotational axes:
-
The transverse sacral axis is at S3 with loading of the
superincumbent weight and with spinal flexion and extension.
Short radius rotational
component perpendicular to the central axis.(Single axis)
-
The transverse acetabular axis with anterior and posterior
pelvic rotation. Long radius rotational component perpendicular
to the central axis.(Single axis)
-
The axis at the pubic symphysis with movement to an asymmetric
pelvis during normal gait - posterior innominate rotation on
the side of loading and anterior pelvic rotation on the side
of the
trailing leg. (Long radius rotational axis on each side =2)
-
The pelvic movement to an asymmetric pelvis rotates the
sacrum laterally toward the side of loading. This lateral sacral
flexion
takes place on an axis perpendicular and central to the sacrum
between the SIJs with a rotational component through both sacroiliac
joints. This creates an oblique axis of rotation with a short
diameter from S1 on the side of loading to S3 on the side of
the trailing
leg. (Axis on each side = 2)
-
Sacral flexion toward the side of loading with movement
on the oblique axis. The short axis rotational component is at
right
angles to the oblique axis. (Axis on each side = 2)
-
The acetabular axis for movement of the pelvis on the femur
or one femur on the pelvis. Axis is from one acetabulum to
the other. The innominate rotates anteriorly in the horizontal
plane
on the acetabular axis when advancing to increase the length
of the step. The long radius rotational component is perpendicular
to the axis. (Axis on each side = 2)
Dysfunction of the sacroiliac joint will cause at least some dysfunction
in all of these pelvic axes.
back
to top
__________
Movement of the Sacroiliac Joint
Demonstration Of Pelvic Movement On The Sacrum At The Sacroiliac Joint
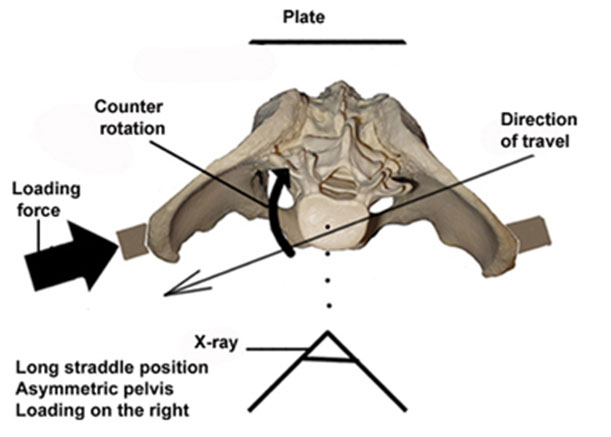
Other than when loading and moving from recumbent to standing, normal sacral movement occurs during normal gait. When the pelvis moves obliquely to the line of travel in order to extend the length of the stride it moves from a position of symmetry into asymmetry. This position with one leg in the extreme forward position and the other in the extreme back position is called the extreme long straddle position. In this position the pelvic bone (innominate bone) on the side of the forward leg (the loading leg) rotates somewhat backward and downward on the sacrum while the pelvic bone on the side of the trailing leg rotates somewhat forward and upward. This movement on the sacrum causes the sacrum to flex laterally toward the side of loading. A force-dependent oblique axis of rotation is created. As the line of gravity is anterior to the sacral axis, the sacrum then moves on that oblique axis to drive counter rotation of the trunk on the loading side in order to decrease the loading forces and protect the head of the femur. This is a controlled instability and it can only occur with movement in the sacroiliac joint.
Many practitioners believe that the sacroiliac joint does not move more than just a few degrees. Even though Smidt measured up to 30 degrees of motion with the patient in the long straddle position, as if taking a long step (). Sturesson measured a subject in the long straddle position and found movement in the sacroiliac joint of only about 5 degrees (). Most physicians accept Sturesson's measurements, which were extremely accurate. In examining the method used by Sturesson I found that he had made an inadvertent error in his positioning that was responsible for a substantial error in the amount of movement measured. Most practitioners accept Sturesson's measurements as accurate, leading to the myth that the sacroiliac joint essentially has no movement and no important function.
I have demonstrated this movement on x-ray and put it on this website rather than publish the information. Although publishing provides some stature it limits access to those professionals who may subscribe to any specific journal.
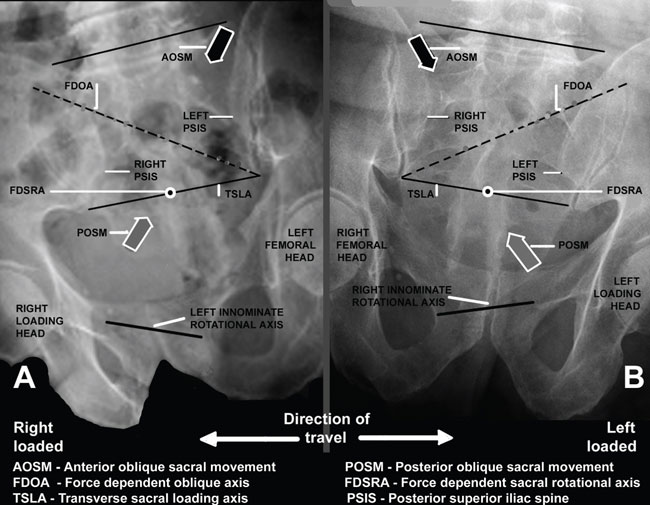
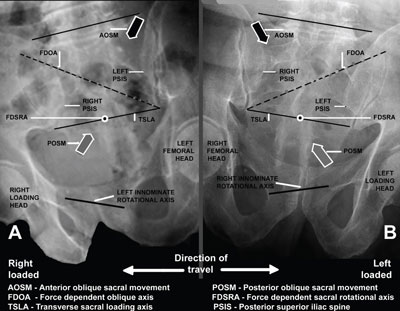
X-rays taken of a pelvis in the long straddle position with counter rotation and with loading to the right and to the left.
 
In order to view innominate movement on the oblique asymmetric pelvis it was necessary to have the front of the pelvis square to the camera, but oblique to the line of travel.
click
to enlarge
DonTigny ©
Movement of the posterior superior iliac spines on the sacrum is obvious and much greater than reported. Clearly, there is ample movement at the sacroiliac joint and not minimal as is commonly believed. This position is clearly static. Dynamic movement would surely demonstrate greater movement than presently observed.
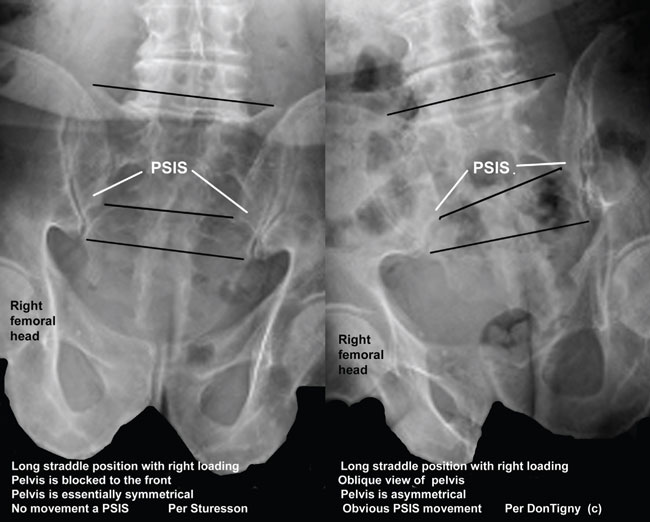
Sturesson had the subject with the direction of travel straight into the camera and with the pelvis perpendicular.

click
to enlarge
DonTigny ©
Sturesson did not have the pelvis in an oblique or asymmetrical position nor did he include counter rotation. Although his measurements were extremely accurate in this position he inadvertently measured some slight movement on the symmetrical pelvis rather than normal movement on the oblique pelvis with counter rotation.
X-rays were taken of the subject in the long straddle position with loading on the right. The x-ray on the left is with the pelvis as per Sturesson, with travel toward the front, no asymmetry and no counter rotation. The one on the right is with the pelvis facing the x-ray, with the direction of travel oblique to the x-ray, the pelvis is asymmetrical and with counter rotation to the right.

click
to enlarge
DonTigny ©
Conclusion: The sacroiliac joint demonstrates ample movement during normal ambulation when the pelvis is oblique to the line of travel and with counter rotation to the right and left.
Acknowledgement
Thanks go to Eric Wilting and John Rosenbaum of the radiology department of Northern Montana Hospital for their expert assistance in this study.
References
1. Smidt GL, McQuade K, Wei S-H, Barakatt E. Sacroiliac kinematics for reciprocal straddle positions. Spine 1995;20:1047-1054
2. Smidt GL. Innominate range of motion. In Vleeming A, Mooney V, Dorman T, Snijders C Stoeckart R, (eds) Movement Stability and Low Back Pain. The Essential Role of the Pelvis. Edinburgh, Churchill Livingstone, 1997: 187-1911.
3. Sturesson R, Selvik G, Uden A. Movements of the sacroiliac joints. A roentgen stereophotgrammetric analysis. ; Spine 1989;14:162-165
4. ; Sturesson B, Vleeming A. A radiostereometric analysis of the movements of the sacroiliac joints in the reciprocal straddle position. In: Sturesson B: Load and Movement of the Sacroiliac Joint. Malmo, Sweden, Rahms Tryckeri i Lund AB, 1999: 75-79
back
to top
|