|
__________
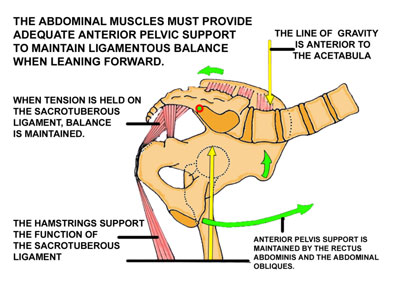
Vulnerability
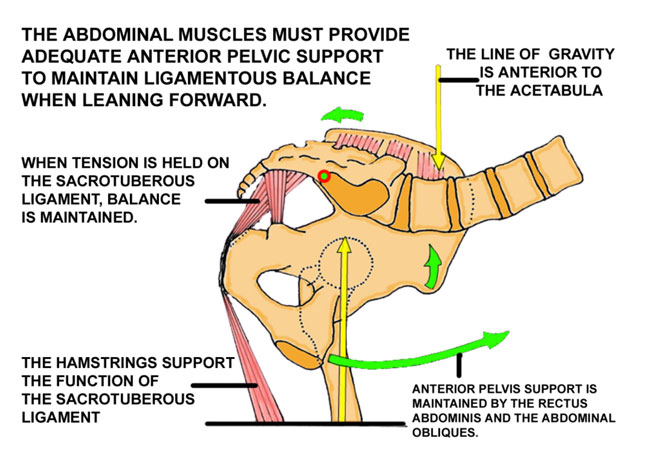
(When leaning forward to
do anything, support of the anterior pelvis by the abdominal muscles
is essential to prevent dysfunction )
The line of gravity moves anterior to the acetabula when lifting,
bending, lowering, shoveling, or
just leaning forward. It may also move forward with a protruding abdomen or
in the later stages of
pregnancy. When it does, the innominates may rotate anteriorly on the sacrum
on an acetabular axis
resulting in a subluxation at the S3 segment.
Holding a strong pelvic tilt when leaning forward in order to maintain the
ligamentous balance
can effectively prevent the onset of low back pain. This is best done with
the rectus abdominis and the abdominal obliques. The transverse abdominis has
only a scant effect on the posterior pelvic tilt.
click to
enlarge
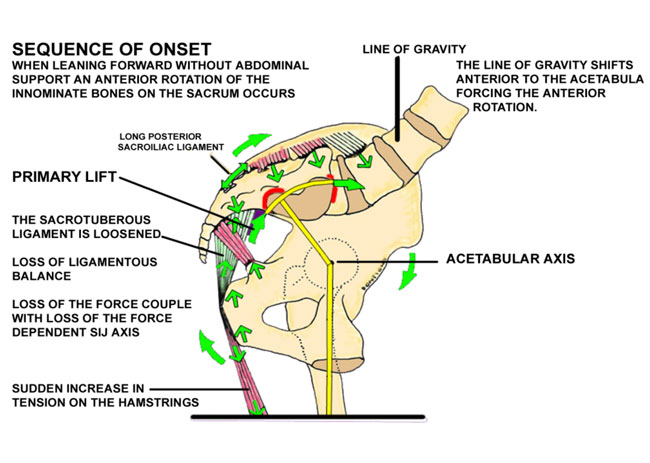
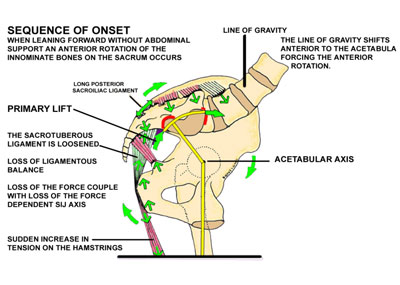
__________ Dysfunction
Sequence of Dysfunction
In the absence of anterior pelvic support when the line of gravity moves anteriorly
the innominates
will tend to rotate cephalad and laterally on the sacrum at S3 and caudad and
laterally on the sacrum at S1. The sacrotuberous ligament is loosened. The ligamentous
balance is disturbed and the innominate bone
will subluxate cephalad and laterally on the sacrum on an acetabular axis.
click
to enlarge
back to top
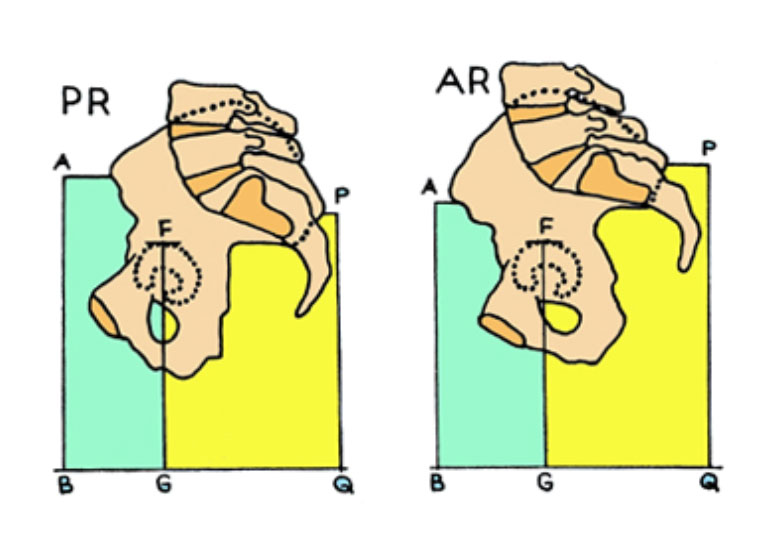
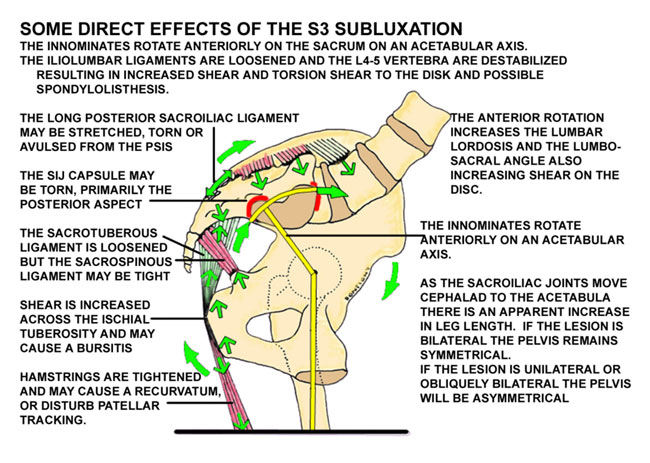
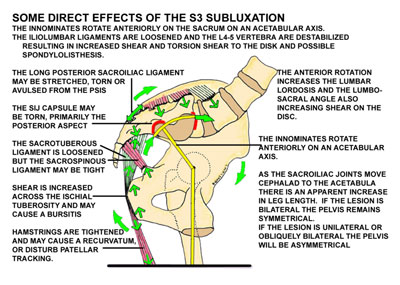
Some Direct Effects of the Subluxation at Ilial S3
With the dysfunction in anterior rotation the SIJs will
move cephalad and anteriorly relative to the acetabular axis
causing an apparent lengthening of the legs. If the dysfunction
is greater on one side the legs will appear to be of unequal
length, but both will still appear longer than normal. The
pelvis will be asymmetrical and the sacral base will be higher
on one side and the sacrum may appear slightly twisted.
Note how the ASIS will appear lower (AB) and the PSIS higher (PQ).
The height of the acetabula will not change. (FG)
This changes to normal symmetry with appropriate correction. |
|
|
back to top
click
to enlarge
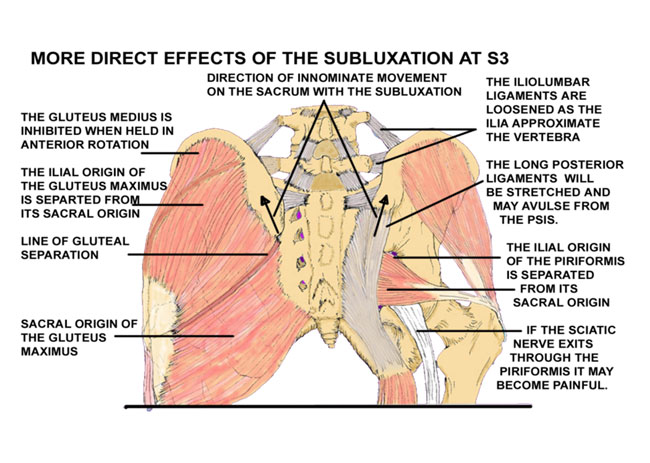
More Direct Effects
The multiplicity of effects from this commonly overlooked subluxation
give the
impression of a multi-factorial etiology.

click
to enlarge
back to top
__________
Associated Conditions
ABDOMINAL PAIN
There may be pain in the abdomen at Baer's SI point described as
being on a line from the
umbilicus to the ASIS, two inches from the umbilicus. One woman
patient had both low back pain
and abdominal pain for four years with removal of both of her ovaries.
She was free of both the
back pain and the abdominal pain immediately with correction of
her SIJs.
BURSITIS
An impairment of the function of the sacral origin of the gluteus maximus may
precipitate a
trochanteric bursitis.
An impairment of function of the piriformis can cause a bursitis beneath the
tendon at the
greater trochanter.
Shear at the ischial tuberosity may cause a local bursitis/tendinitis with pain
and tightness in
the biceps femoris.
BUTTOCK PAIN
Buttock pain at the PIIS is at the location of the dysfunction at S3 and is the
location of the
conjoint origin of the piriformis muscle.
CHANGES IN GAIT
With a bilateral subluxation the horizontal pelvic swing is shortened. With a
unilateral
subluxation and apparent long leg you will ambulate with a high iliac crest on
the more
painful side.
With the compromised bilateral subluxation at S3 you will ambulate with a short
leg on the
more painful side. Functional lateral sacral flexion, function of the piriformis
and the sacral origin
of the gluteus maximus are impaired.
Dorman described inhibition of the gluteus medius with anterior innominate rotation.
The
resultant weakness in the abductors may allow the pelvis to drop prematurely
on the contra lateral
side increasing loading forces and shortening the length of the step.
Dannanberg described an inhibition of the peroneus longus with SIJD causing a
hallux limitus
(a rigid big toe) relieved with orthotics. The peroneus longus supplies up to
18% of the strength to the
sacrotuberous ligament through the kinetic chain.
DESTABILIZATION OF THE LUMBAR VERTEBRA
The anterior innominate rotation will loosen the iliolumbar ligaments destabilizing
L4-5, S1 and increasing shear and torsion shear to the disks. L5 tends to shear
anteriorly on S1 and may initiate or increase a spondylolisthesis. Any anterior
shearing movement of spondylolisthesis will tend to tighten
the iliolumbar ligaments again, which may prevent reduction of the subluxation
at the S3 segment.
FASCIAL TIGHTNESS
Increases in fascial tightness may occur with increased loading forces that may
cause some
stiffness and limit hip motion or passive straight leg raising.
GROIN PAIN
Pain in the groin may be caused from a vertical shift of the pubic bone at the
symphysis if
the SI dysfunction is more on one side than the other. If motion in the SI joints
from SIJD
is blocked posteriorly the forces of asymmetry when walking may also cause pain
anteriorly at the
pubic symphysis.
KNEE PAIN
The sudden release of the balanced loading via the biceps femoris can strain
the lateral
capsule of the knee or may subluxate the head of the fibula.
INCREASED PAIN WITH COUGHING OR STRAINING
As the innominate bones will tend to separate and spread with this dysfunction,
any increase in intraabdominal pressure such as caused by a sudden cough or straining
with a bowel movement
will tend to further increase the spreading and thus increase the pain.
INCREASED SHEAR TO THE DISK
The anterior inclination of the pelvis with SIJD will cause a lumbar lordosis
and an increase
in the lumbosacral angle, increasing shear to the disk and inhibiting the multifidus
muscle.
MUSCLE INHIBITION
Dorman found a positional inhibition of the gluteus medius when the innominate
in held in
anterior rotation.
Dananberg found an inhibition of the peroneus longus with SIJD causing a functional
hallux
limitus.
MUSCLE SEPARATIONS
The gluteus maximus, the piriformis and the iliacus muscles each have origins
on both the
sacrum and the ilium. SIJD can stress these conjoint origins and cause pain in
any or all of these
muscles.
MYOFASCIAL PAIN OR FIBROMYOSITIS
If the SIJ is not corrected the force couple will not function properly. Loading
will be increased to the femoral head and can cause pain down the legs and up
the back giving the impression of fibromyositis.
PAIN ON SITTING
When standing, weight bearing on the head of the femurs has a buttressing effect
that is lost
when sitting. Weight bearing is on the ischial tuberosities when sitting, which
tends to loosen the sacrotuberous ligaments.
PELVIC CONGESTION
A pelvic obliquity may increase tension to the floor of the pelvis. Pelvic congestion
plays a
major role in female patients with dysmenorrhea, ovarian cysts, and premenstrual
syndrome as well
as in male patients with prostatitis and prostatodynia. Pain may be referred
into the groin and cause a pseudoepidymitis. May cause incontinence, especially
in women, relieved with correction.
RENTS IN THE SIJ CAPSULE
Fortin found rents in the capsule might leak synovia to the lumbo-sacral plexus,
to the root
of the fifth lumbar nerve and into the body of the psoas muscle and cause neurological
symptoms.
Leaking synovia may become encapsulated and form cysts on the sacroiliac joint.
PIRIFORMIS SYNDROME
Separation of the sacral origin of the piriformis muscle from its ilial origin
at the superior
margin of the greater sciatic notch at the PIIS can cause pain in the piriformis
muscle.
SACRAL TORSION
Any apparent sacral torsion will be corrected with correction of the innominate
bones on the sacrum.
It is not necessary and sometimes counter productive to attempt direct correction
of sacral torsion.
SCIATIC NERVE PAIN
The sciatic nerve is also stretched with this anterior rotation and when combined
with the
irritation from the separation of the piriformis muscle the resultant neuritis
is to be expected.
Sciatic neuritis is often present in the absence of disk herniation.
SCOLIOSIS
If the dysfunction is asymmetrical it will unlevel the sacral base and may cause
a lumbar
scoliosis with bulging disks. If this occurs in pre-pubertal children the asymmetric
sacral base can
cause asymmetric development.
SENSORY CHANGES
When the innominates rotate downward anteriorly on the sacrum, the nerve roots
may be
stretched. When the nerve root gets stretched, it gets smaller and compression
deformity of the
nerve roots occurs. Total mechanical block occurs before 15% elongation. The
dorsal roots are
more susceptible to stretch that the ventral roots, hence changes in sensation
are more likely to
occur. Pudental Nerve Entrapment: Pain referral patterns may simulate entrapment
of the pudental
nerve. Correct the SIJ first and then reassess.
TIGHT PSOAS
The anterior inclination of the pelvis will stretch the psoas muscle and gives
the appearance of tight hip flexors. Stretching the hip flexors will increase
the dysfunction.
Correction of the
dysfunction will take the stretch off of the hip flexors.
back to top
|